
Doctors have no idea how much their patients are suffering. That's about to change.
by Susannah Locke on October 15, 2014
Ally Niemiec could have lost a kidney because doctors didn't believe she was in pain. It was last fall, and one of at least a dozen times that her rare kidney disease had sent her to the emergency room. She recognized the pain. She knew something was wrong.
But when she turned up in an Atlanta emergency room that Saturday afternoon, vomiting and doubled over, no one believed her. They looked at her pain medication records and decided she had a drug abuse problem.
"They told my mother that I needed to go to rehab and was a drug addict," she says. The hospital wouldn't give her any narcotic pain medication and refused to do an x-ray, ultrasound, or CT scan.
That time, Niemiec was lucky enough to have other options. She left for another hospital, where they treated her pain and then removed her kidney stone the next morning.
This discouraging experience was nothing new. For many years, she was used to doctors not trusting her. "There's nothing more horrific than a doctor looking you in the eye and saying there's nothing wrong with you when you're in debilitating pain"
One problem has been that her kidney disorder, renal tubular acidosis type 1, is described in medical journals as not painful. But to her, it was. Since she was 13, she's had about 100 kidney stones and 18 surgeries to remove them. At one point, her pain was so bad that she couldn't drive and had to leave her job. She went from doctor to doctor trying to get help. When her pain got really bad, she didn't find adequate treatment for three long years.
"There's nothing more horrific than a doctor looking you in the eye and saying there's nothing wrong with you when you're in debilitating pain," she says. "To me, it's a form of torture."
Eventually, she got a spinal cord implant that uses electrical signals to block her kidney pain. Now she's 24 years old and works at a tech startup. But many others continue to suffer.
Approximately 100 million Americans have chronic pain. That's about a third of the population. Yet the most cutting-edge test for pain is a doctor holding a piece of paper with a bunch of frowny and smiley faces on it or asking you how bad you feel on a scale of 1 to 10, with ten as the worst pain imaginable. It seems a much better test of imagination than of pain.
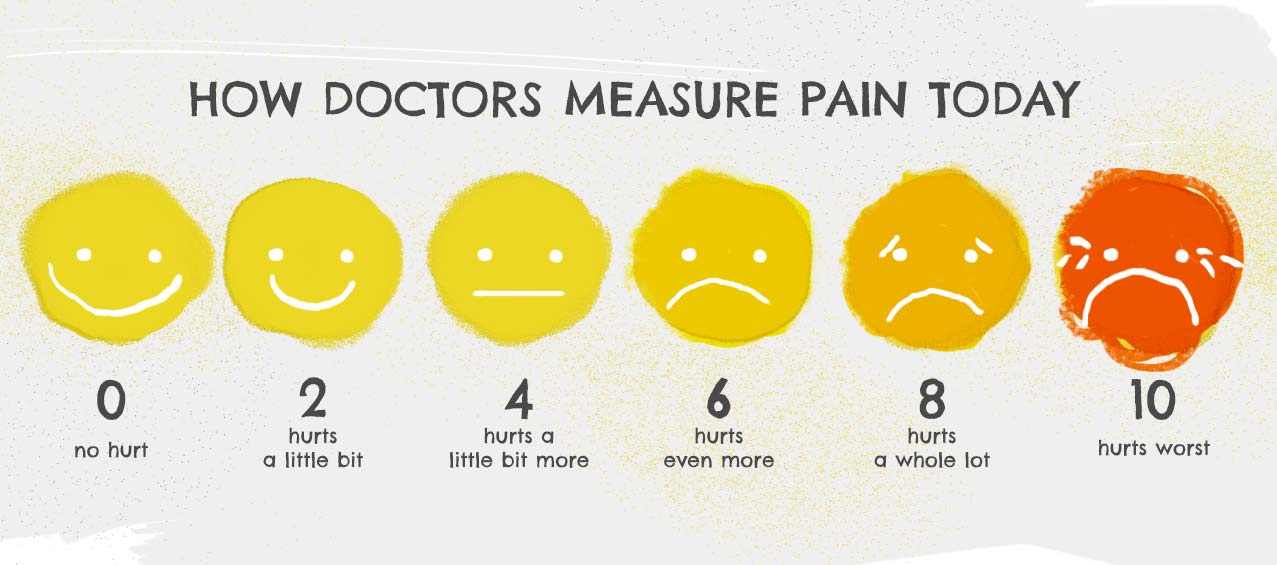
And as Niemiec can attest, the subjectiveness of the scale causes problems — it only works if the doctor believes you, and relying only on trust can threaten people's lives.
There must be a better way to test if someone is in pain. "That would completely have changed my experience," Niemiec says. "It could have saved me three years of my life."
Right now, such a test doesn't exist. But it's looking likely that it might someday soon. In several key studies, scientists have used brain-scanning machines to accurately predict if someone is in pain.
A more objective pain test could transform pain medicine and lead to new treatments for people who suffer. It could weed out people lying in order to get drugs. And it could prove to doctors that people like Niemiec are really in pain.
But this new technology also raises all kinds of ethical and legal questions. It might also end up as faulty mind-reading that could be used to deny care and insurance coverage to those who are truly in distress.
What is pain?
"Pain is so wonderful because it is so bad," says Sean Mackey, the chief of pain medicine at Stanford's medical school, who was the first to show that pain can be gauged using a brain scan. "It keeps us out of harm and out of danger."
Mackey's right: pain teaches people to stay away from hazards and tells them when they're injured or sick. It trains us to keep our hands away from hot stoves. It lets us know when our appendix has burst. Or when we're having a heart attack. Pain is so important that people who cannot feel pain encounter repeated injuries and have shorter life spans.
Despite pain's importance, it is quite difficult to define. And that difficulty underlies much of the disagreement about whether objective pain testing is even possible.
Today, pain is understood as a type of subjective experience. The International Association for the Study of Pain states that pain is "An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage."
So although the mechanisms for what usually causes pain — certain receptors on certain neurons — are fairly well known, pain is still not defined as a physical thing that your body does. Your neurons could be firing off pain signals like crazy, but as long as you don't feel pain (like if you've popped an Advil or are under anesthesia), you're not in pain. If you feel pain, you are in pain.
But brain imaging can put an image to the invisible.
It can give them something to see.
Why the world needs a better pain test
Mackey, the Stanford pain specialist, got his PhD in electrical engineering and also an MD. "Coming out of medical school, you probably couldn't find anyone more mechanistic or linear in their thinking than me," he says. "I ended up going into pain medicine because I was intrigued about the opportunities of really making a difference in people's lives."
Working with pain patients, he often found himself using needles to block pain. (One common treatment for chronic pain is a temporary injection of anesthetic into the body, which stops pain signals from reaching the brain.) But it wasn't working for everyone. "There was large numbers of people that I wasn't helping with that approach," he says. "What really was helping them was listening to them, hearing about their fears, their anxieties, their beliefs about their pain."
Those observations got him interested in the brain side of things, the psychology side, and how things like anxiety, fear, and empathy influence pain. "It was around this time that this field of neuroimaging was being established, which allows us to open up windows into people's brains to see where pain is processed and perceived."
He wanted to use the technology to learn about how people experience pain differently and how thoughts and emotions affect pain, hoping to be able to better tailor therapies to people for better treatment. Along the way, it began to seem possible to create a test that would correlate with someone's pain levels.
A pain test could help all kinds of people. One main group is those who can't speak for themselves. For example, even into the 1980s, some doctors didn't believe that babies felt pain and so routinely did surgery on them using just muscle relaxants to keep them still. And today, some people can't tell others what they're feeling, including small children, some adults with developmental disorders, and people in coma.
And even among people who can communicate fully, not everyone's word is regarded as truth. Researchers have documented discriminatory patterns in how health-care workers treat pain. Women are more likely to have their pain dismissed as not real. And one study found that female emergency room patients with abdominal pain were less likely to be given strong pain meds than men were. Papers have found similar phenomena for racial minorities.
And until the last couple of decades, doctors thought that many people with chronic pain were faking it. Roger Fillingim is a psychologist at the University of Florida who studies pain. He describes patients saying that just the feeling of a long-sleeved shirt on their arm was painful: "We used to call that crazy." Now, doctors know that a lot of chronic pain is actually real. For example, fibromyalgia, which causes pain throughout the body, was in the crazy category, too. Now it's known to affect roughly 15 million people in the United States.
The problems with pain medication
Drug abuse is another reason a better pain test could come in handy. That abuse has led narcotic painkillers to become more tightly controlled in recent years, sometimes so tightly that people with real pain problems have trouble getting their medication.
There's no question that there's a prescription-drug abuse problem in this country. Each year, more people die in the United States from prescription painkillers than from heroin and cocaine combined. And some, but not all, of the people abusing these drugs are people who do not have an actual pain problem.
One recent review on the topic found that about 20 percent of chronic pain patients given opiate drugs long-term had either none of the drug or a non-prescribed opiate in their urine during screening tests, which suggests that they might be selling or giving the drugs away rather than taking them responsibly. (The study also found that very few — 3 percent — of all of the patients personally ended up with an addiction or abuse problem related to these drugs. If patients with a history of drug abuse are excluded, this number drops below one percent. However, screening people out doesn't always happen in today's hectic health-care environment.)
It's difficult to balance what regulations will get pain meds to patients who need them while keeping them from people who don't. You can see where these objectives collide in the recent battle over Zohydro ER. This new drug is an extended-release version of the opiate hydrocodone and the only hydrocodone for sale without another drug in it.
It's also somewhat analogous to OxyContin, which became a preferred drug of abuse in the late 1990s and early 2000s — at least until 2010, when its manufacturers made OxyContin difficult to snort or inject, with pills that were hard to crush and that turn into a gel when wet. "If you could somehow measure pain, would that be helpful? It would be helpful to me because I want to know if my patients are legitimate."
However, Zohydro ER, like every opiate on the market except for OxyContin, has no such anti-abuse features built into its pill. For some with chronic pain, it's their only chance for relief. To others, it's death in a bottle.
In October 2013, the FDA approved Zohydro ER against the recommendation of its independent advisory panel. In the spring of 2014, Massachusetts governor Deval Patrick banned it, but a judge struck the ban down just a month later. And in August, several governors petitioned the US Department of Health and Human Services to undo the decision.
Concerns about abuse have also led to changes in regulation and enforcement that pressure doctors, wholesalers, and pharmacists to give out fewer narcotic painkillers.
For example, in Florida, crackdowns to combat a previously growing problem with pain-medication deaths has made it difficult for legitimate pain patients to actually get their prescribed medication, says Jeffrey Fudin, a pharmacist who specializes in pain treatment and is an adjunct associate professor at Western New England University.
A better pain test is one thing that could help real pain patients prove themselves — and weed out the liars. "If you could somehow measure [pain] would that be helpful? It would be helpful to me because I want to know if my patients are legitimate," Fudin says.
The research on brain imaging
Recent advances in brain-imaging technology have shown that the mind's secrets are sometimes surprisingly readable. For example, some researchers have used brain scanning to guess with some accuracy what shapes people are looking at or what type of object they were dreaming of: a building, a car, a person.
The main technique researchers are using is functional magnetic resonance imaging, or fMRI. An fMRI machine employs a giant magnet that can read where blood is in the brain. And because blood flows more to active brain areas, an fMRI scan can measure brain activity.
In the past few years, researchers have published studies showing that fMRI could determine whether someone is in pain.
In 2011, in a small study of 24 people, Mackey's group used advanced computer algorithms to show whether someone was receiving a painfully hot stimulus to his or her forearm with 81 percent accuracy. The observed differences in brain activity weren’t clustered in only one area, but in many, many places across the entire brain.
A pain test could help all kinds of people. One main group is those who can't speak for themselves.
In 2013, a paper led by Tor Wager, a neuroscientist at the University of Colorado Boulder, confirmed those findings in a bigger study published in a very prestigious journal: The New England Journal of Medicine. It involved 114 participants and correctly guessed whether someone was in pain about 95 percent of the time. Even more impressive was that the brain patterns seemed somewhat universal — that is, the algorithms were developed on one set of volunteers and then worked on another set that had never been scanned before.
Then in 2014, Mackey published another paper that looked at patients with chronic back pain, using still MRI images to examine brain structures rather than brain activity. He was able to produce an algorithm that guessed with 76 percent accuracy whether or not a brain was from a chronic back pain patient. A similar study published the same year identified people who had chronic pelvic pain with 73 percent accuracy.
Still images of brain structure like these could someday help chronic pain patients justify their condition, even though they don't show brain activity itself.
All of these new studies are still firmly in the realm of science, not medicine. These tools are not ready for use on patients to determine a course of treatment. Mackey estimates that that might be 10 years away.
The tests can't yet accurately predict someone's exact level of pain. And they've only been demonstrated within the confines of well-controlled laboratory studies.
In addition, most researchers don't believe that there's just one pain brain-activity pattern, but that different kinds of pain will end up producing different patterns. So, touching something hot might look different than the muscle pain of fibromyalgia, which might look different than chronic back pain. And that means that a lot more research will be needed before such technology could be used on the wide variety of painful health issues that exist.
The problems with an 'objective' pain test
Both Mackey and Wager see a lot of potential in using brain imaging as a research tool to better understand the various causes and types of pain — and to develop new ways to treat it. They think that such scans should only be used to confirm someone's pain, but never to go against their word and deny that they're in pain when they say that they are. That's because pain is defined as a subjective experience. And the brain scan is objective. So, to them, the brain scan is merely an objective marker of possible pain.
Another reason for that stance is that a person could be feeling a kind of pain that they haven't found the brain signature for yet. "It might not look like other people's pain, but it might be their pain," says Wager.
And, says Mackey, "There is the potential for abuse. There's always the potential for people misusing this technology for insurance purposes to deny care."
However, both researchers do support using the technology someday on people who can't say if they're in pain or not, like babies or some people with developmental disabilities. Because any evidence is better than nothing at all.
Another problem is that pain might be something that cannot be reduced to a bunch of neurons firing. "Some people believe that pain isn't simply some sum or algorithm of brain activity, it's an emergent property of brain activity," says Fillingim. "And maybe we won't figure out how the experience of pain emerges from some pattern of brain activity. And maybe the formula is different for different people."
"Could we similarly look at someone's brain and tell you how happy they are, how satisfied with life?" he asks. "These are all pretty high level experiences."
Another problem could come from brain-scan pain tests getting used in court. Some people approximate that awards for pain and suffering make up about half of personal injury damage awards. So there's big money on the line. "The legal system has a tremendous need for more objective ways of measuring pain," says Adam Kolber, a professor at Brooklyn Law School who has written extensively about the future ethical and legal implications of pain testing. "There is the potential for abuse. There's always the potential for people misusing this technology for insurance purposes to deny care."
He's not that concerned about how pain tests will be used in the long run. He notes that there are standards in place to stop new technology from becoming admissible evidence until it's fully developed. And he focuses on the positive side of what the technology could do: "This is a possibility of better compensating people who are in pain. I think that's promising."
But not everyone agrees. And Mark Sullivan is one of them. He's a psychiatrist and bioethicist at the University of Washington who specializes in treating patients with chronic pain. He's been one of the most vocal opponents of the drive to find objective measures of pain.
He's debated both Mackey and Wager in person at pain research meetings and debated on paper in the Journal of Pain in 2013. And he says he's concerned about people who are truly ill being denied workers' compensation and social security because nothing can be found on a brain scan: "You could easily see a situation where someone says, ‘Well, I can't work because I have terrible back pain.' And you stick them in an MRI scanner and it's ‘I don't see any evidence that you're in pain. So we're not going to give you disability payments anymore.'"
Whether it leads to good or bad outcomes, computing power, fMRI resolution, and data from patients will keep increasing. Technology will march on, and someday, someone is going to start selling something called an objective pain test, whether or not that's actually what it's capable of.
And no matter how accurate the test is or isn't, the images it produces could help pain become a more visible problem in health care. Pain isn't something that someone can see, like a physical wound. It can take numerous forms, making it easier for medical practitioners to ignore.
44-year-old Californian Elizabeth Schenk is one of the many patients who've had doctors ignore her agony. She used to be a pilates instructor, but her chronic pain has brought her into a new career counseling people with pain problems. At its worst, her pain has been excruciating: "like someone was dragging a knife down my thigh," and "like someone taking a hammer to my thumb," and "a chisel to my spine."
"What I've experienced in the medical world is that if they don't see anything, they won't do anything," she says. But brain imaging can put an image to the invisible. It can give them something to see.
http://www.vox.com/2014/10/15/6895171/how-doctors-measure-pain-brain-scan-fmri
No comments:
Post a Comment
All comments welcome but advertising your own service or product will unfortunately result in your comment not being published.